|
|
|
>>Others
About The Prostate |
|
|
|
2010
Annual Report on Prostate Diseases |
Pathophysiology |
|
More deaths if no prostate cancer
therapy |
Prostatic Adenocarcinoma |
|
Calcium consumption may up prostate
cancer risk |
Dog Sniffs Out Prostate Cancer in
Small Study |
|
Mixed Fruit Juice reduces
Prostate Cancer Risk |
Drinking Green Tea Daily lowers
Prostate Cancer Risk |
|
Why you should consider a
prostate cancer PSA test today |
|
What Dennis Hopper's Death Can Teach
Us About Prostate Cancer |
|
Prostate cancer patients with
low-risk tumors could hold off
treatment |
|
What Can Go Wrong With the Prostate:
Cancer, BPH, and Prostatitis |
|
Ultra-sensitive test to tell
prostate cancer patients if they are
cured after operation |
|
Sound waves prostate cancer
treatment may have lesser side
effects on the patient |
|
Prostate Cancer Hormone Therapy May
Prove Successful in Treatment of
Surgery-Resistant Cancer |
| |
| |
|
2010
Annual Report on Prostate Diseases |
Prostate disorders usually
develop after age 50, but some men
experience them at a younger age.
The three most common conditions are
prostatitis, benign prostatic
hyperplasia (BPH), and prostate
cancer. Although they share some of
the same symptoms, they are very
different. Treatments vary, too. For
example, two men with prostate
cancer might opt for treatments as
divergent as radical surgery and
doing nothing at all. Even getting
screened for prostate cancer, which
seems like it would be a no-brainer,
requires thoughtful consideration.
That’s because most men usually feel
compelled to undergo treatment if
cancer is diagnosed, risking
complications like impotence and
incontinence that can undermine
quality of life.
Whether you are considering
medication for BPH or erectile
dysfunction, or debating between
radiation therapy and surgery for
prostate cancer, you need to review
your options carefully. This report,
which provides an objective
assessment of the risks and benefits
of various procedures, can help.
More than a primer on the most
common prostate conditions, this
unique publication includes
roundtable discussions with experts
at the forefront of prostate cancer
research; assessments of different
therapies from Harvard Medical
School doctors; interviews with
patients about their treatment
decisions; and the latest thinking
on complementary therapies. It also
includes helpful tips on managing
and treating erectile dysfunction
and impotence caused by prostate
disease therapies.
Prepared by the editors of Harvard
Health Publications in consultation
with Marc B. Garnick, M.D., Clinical
Professor of Medicine, Harvard
Medical School, and
Hematology/Oncology Division, Beth
Israel Deaconess Medical Center. 136
pages. (2010)
A year of advances and breakthroughs
in prostate disease
What made news in 2009
Monitoring prostate health
A look at the prostate and some
tests you might need
Prostate enlargement (benign
prostatic hyperplasia)
Getting this “going”―and
“growing”―problem under control
Inflammation of the prostate (prostatitis)
Help for an all-too-common condition
Prostate cancer
What you need to know at every stage
of the disease
Erectile dysfunction and
incontinence
Some solutions to consider
Complementary therapies for prostate
disease
What works ― and what doesn’t
Take charge of your condition
Participate in a clinical trial or
support group
Resources
Organizations and publications you
can turn to for more information
Glossary
Definitions of medical terms used in
this report
Searching PubMed in five easy steps
How to access the studies cited in
this report
PSA screening: What makes sense?
Making decisions when questions
remain
Since its introduction in the late
1980s, the prostate-specific antigen
(PSA) test has been hailed as a way
to detect prostate cancer in its
earliest, most curable stage. It has
been called one of the most
important tests a man can have. So
why are many experts now stepping
back, and even discouraging the use
of widespread PSA screening?
The shift comes on the heels of a
growing body of evidence that shows
the benefits of PSA screening may
not outweigh the potential harm of
unnecessary treatment. PSA screening
has always been somewhat
controversial. That’s because PSA
tests often alert doctors to the
presence of cancer, but there is no
precise way to determine,
definitively, whether the cancers
detected would have ever caused
symptoms or harm during a man’s
lifetime. One study estimated
overdetection to rise with age, from
27% at age 55 to 56% by age 75.
Despite this, to be on the safe
side, most men with elevated PSA
levels will opt for treatment,
frequently suffering side effects
such as incontinence and impotence.
Increasingly, there are questions
about the effectiveness of PSA
screening for prostate cancer. Just
how many lives are actually being
saved? And is the emotional and
physical toll on the millions of men
who are being overdiagnosed and
overtreated worth it?
Two long-awaited studies―one
conducted in the United States and
the other in Europe―were supposed to
help settle the debate over the
value of PSA testing. Instead, the
trials, published in The New England
Journal of Medicine in March 2009,
seemed to come to opposite
conclusions. The Prostate, Lung,
Colorectal, and Ovarian (PLCO)
Cancer Screening Trial reported no
survival benefit with PSA screening
and digital rectal examination, but
the European Randomized Study of
Screening for Prostate Cancer (ERSPC)
found a 20% reduction in prostate
cancer deaths. The ERSPC study
estimated that for every life saved,
48 men are treated and nearly 1,068
men are screened.
Although experts are somewhat split
on the value of PSA tests as a
screening tool, there is widespread
agreement on two major points:
overdiagnosis and overtreatment
rates are far too high, and there is
an urgent need to refine PSA testing
to be a more effective screening
tool. The principal investigator of
the Prostate Cancer Prevention Trial
and his colleagues wrote an
editorial in The Journal of the
American Medical Association in
October 2009 that took a closer look
at the issues. They pointed out that
while the amount of prostate cancer
diagnosed has risen dramatically
since PSA testing began, there has
not been a proportional decrease in
the number of men with metastatic
tumors. It appears screening may be
detecting a disproportionate number
of lower-risk cancers, while missing
many of the most aggressive tumors,
which may advance too rapidly to be
found with periodic testing.
The debate over the effectiveness of
PSA screening has quickly filtered
into the offices of general
practitioners and urologists. On a
daily basis, confused men are asking
their doctors: “Should I have a PSA
test or not?”
To help men sort through the latest
thoughts on PSA screening, the
editors of Harvard Medical School’s
2010 Annual Report on Prostate
Diseases invited three Harvard
experts to participate in a
roundtable discussion on screening.
The panelists represent physicians
on the front lines of the debate… |
|
Article
Source:http://www.health.harvard.edu/special_health_reports/Prostate_Disease.htm |
|
Back To Top |
|
What Can Go Wrong With the Prostate:
Cancer, BPH, and Prostatitis |
For most young men, the prostate
falls into the category “obscure
body parts” that includes the
spleen―that is, it’s in there
someplace, it probably does
something useful, but it’s best
dealt with on a need-to-know basis.
Unfortunately, most men are going to
need to know about the prostate
sometime, because this little gland
is the source of three of the major
health problems that affect men:
■Prostate
cancer, the most common major cancer
in men
■Benign
enlargement of the prostate (BPH, or
benign prostatic hyperplasia), one
of the most common benign tumors in
men and a source of symptoms for
most men as they age
■Prostatitis,
painful inflammation of the
prostate, the most common cause of
urinary tract infections in men
Worse, because there’s no “statute
of limitations” on prostate
problems, some men are unlucky
enough to endure more than one of
these disorders. For example, having
BPH or prostatitis doesn’t mean a
man won’t have further
difficulty―either a return of
symptoms or a new problem entirely,
such as prostate cancer.
When it comes to making the
diagnosis of prostate cancer and
planning treatment, the other
prostate disorders must be
considered, too. So it’s important
that men know about all three
problems―what they are, how they are
treated, and their telltale
symptoms.
Fortunately, effective treatment and
relief of symptoms is available for
all three prostate disorders. Even
prostate cancer, when caught early,
is treatable―generally without
causing loss of urinary control or
sexual function. In fact, many
prostate cancers may not need to be
immediately treated and can be
safety followed under a program of
active surveillance.
Clinical trials are ongoing to
understand which cancers need to be
treated aggressively with surgery or
radiation, and which can be observed
with deferred therapy or no therapy.
For the first time ever, we are very
close to understanding how to keep
advanced cancer in check, perhaps
even for years. |
|
Article Source:
http://www.pcf.org/site/c.leJRIROrEpH/b.5813303/k.CDC2/What_Can_Go_Wrong_With_the_Prostate_Cancer_BPH_and_Prostatitis.htm |
|
Back To Top |
|
Calcium consumption may up prostate
cancer risk |
Calcium consumption ― even at
relatively low levels and from
non-dairy food sources such as soy,
grains and green vegetables ― may
increase prostate cancer risk among
Chinese men, according to a new
study.
The study has been published in
Cancer Research, a journal of the
American Association for Cancer
Research.
"Our results support the notion that
calcium plays a risk in enhancing
the role of prostate cancer
development," said lead researcher
Lesley M. Butler, Ph.D., assistant
professor of epidemiology at
Colorado State University, Fort
Collins, Colo. "This study is the
first to report an association at
such low levels and among primarily
non-dairy foods."
Some studies conducted in North
American and European populations
have linked high consumption of
dairy products to an increased risk
of prostate cancer. A few studies
have suggested that calcium in milk
is the causative factor, however the
evidence is not clear.
In an Asian diet, non-dairy foods
like tofu, grains and vegetables
such as broccoli, kale and bok choy
are the major contributors of
calcium intake. Therefore, Butler
and colleagues speculated that
people who are exposed to those
calcium-rich food sources in an
Asian diet may also be at increased
risk for prostate cancer.
Using data from the Singapore
Chinese Health Study, the
researchers evaluated whether
dietary calcium increased prostate
cancer risk in a population of
27,293 Chinese men aged 45 to 74
years, with low dairy consumption.
The study was restricted to men who
belonged to two major dialect groups
of Chinese people living in
Singapore: the Hokkiens and the
Cantonese.
Participants completed a food
frequency questionnaire to assess
their diet over the past year. Of
these men, 298 were diagnosed with
incident prostate cancer.
Butler and colleagues at Colorado
State University, the National
University of Singapore and the
University of Minnesota assessed the
participant''s diet at baseline.
Since it is suggested that calcium
is absorbed more so in smaller
individuals, the researchers
accounted for body mass index (BMI)
in this Chinese population.
Results showed a 25 percent
increased risk of prostate cancer
when comparing those who consumed,
on average, 659 mg vs. 211 mg of
total calcium a day, according to
the study.
Major food sources of calcium in
this population consisted of:
vegetables (19.3 percent), dairy
(17.3 percent), grain products (14.7
percent), soyfoods (11.8 percent),
fruit (7.3 percent) and fish (6.2
percent). However, the researchers
stress that there was no positive
association with prostate cancer
risk and any one particular food
source.
Among men with less than average BMI
(median BMI was 22.9 kg/m2), the
researchers found a twofold
increased risk of prostate cancer.
"It was somewhat surprising that our
finding was consistent with previous
studies because nearly all of them
were conducted among Western
populations with diets relatively
high in calcium and primarily from
dairy food sources," Butler said.
|
|
Article Source: http://timesofindia.indiatimes.com/life/health-fitness/health/Calcium-consumption-may-up-prostate-cancer-risk/articleshow/6002588.cms |
|
Back To Top |
|
Dog Sniffs Out Prostate Cancer in
Small Study |
TUESDAY, June 1 (HealthDay News) --
New research suggests that dogs can
sniff out signs of prostate cancer
in human urine, adding to the
ongoing debate over the
disease-detecting powers of man's
best friend.
Some scientists have questioned
similar reports of dogs with such
diagnostic powers in recent years,
but the lead author of this latest
study said the findings are
promising and could lead to better
cancer-sensing technology.
"The dogs are certainly recognizing
the odor of a molecule that is
produced by cancer cells," said
French researcher Jean-Nicolas Cornu,
who works at Hospital Tenon in
Paris.
The problem, he said, is that "we do
not know what this molecule is, and
the dog cannot tell us."
Still, the report could represent a
significant development since cancer
often goes undetected until it is
too late to treat.
The detection of prostate cancer has
been particularly controversial.
Some researchers think many patients
are treated unnecessarily because
existing tests of prostate-specific
antigen (PSA) aren't accurate enough
and fail to distinguish between
dangerous and harmless cancers.
Urine tests can turn up signs of
prostate cancer, Cornu said, but
miss some cases. Some types of
molecules give a distinct odor to
urine, "but today there is no means
to screen odors from urine and
separate them," he said, and no way
to link them to cancer.
Enter the dog, whose powers of smell
are far greater than those of
humans.
For this study, two researchers
spent a year training a Belgian
Malinois shepherd, a breed already
used to detect drugs and bombs.
The dog was trained to differentiate
between urine samples from men with
prostate cancer and men without.
Ultimately, researchers placed
groups of five urine samples in
front of the dog to see if it could
identify the sole sample from a man
with prostate cancer.
The dog correctly classified 63 out
of 66 specimens.
If the findings hold up in other
studies, they'll be "pretty
impressive," said urologist Dr.
Anthony Y. Smith, who was to
moderate a discussion on the
findings Tuesday at the American
Urological Association annual
meeting in San Francisco.
Skeptical researchers are concerned
about factors that could throw off
the results, said Smith, chief of
urology at the University of New
Mexico. Among other things,
scientists wonder if the animals
used in such studies pick up on
subconscious signals from
researchers.
Still, in this study, it's hard to
imagine anything "other than the
dogs somehow being able to smell
something that we don't smell,"
Smith said.
If these findings are valid, they
could lead to the development of
more accurate tests that don't
require unnecessary biopsies, Smith
said.
The next steps are to determine
precisely what the dogs are sniffing
and to develop an "electronic nose"
to detect it, Cornu said. Other dogs
are already being trained, he said.
Could doctors and hospitals employ
dogs and researchers to detect
prostate cancer? Cornu said that's
possible, but it could cost as much
as hiring two full-time scientists. |
|
Article Source: http://www.businessweek.com/lifestyle/content/healthday/639647.html |
|
Back To Top |
|
Drinking Green Tea Daily lowers
Prostate Cancer Risk |
Japanese scientists suggest that
drinking daily five or more cups of
green tea could halve the risk of
developing advanced prostate cancer.
According to the article published
in the American Journal of
Epidemiology, there was a 50 percent
lower risk of having advanced
prostate cancer in men who drank
five or more cups of green tea daily
compared with those who had less
than a cup.
Findings show while drinking green
tea lowers the risk of advanced
prostate cancer; it is not
associated with localized prostate
cancer.
Researchers claim that a substance
called catechin in green tea is
responsible for reducing cancer risk
by curbing testosterone levels which
cause prostate cancer.
The study suggests that the lower
incidence of prostate cancer in
Asians may be linked to the higher
consumption of green tea.
Previous studies had reported
various health benefits for the
green tea catechin including reduced
heart attack and cancer risks.
|
|
Article Source: http://www.healthjockey.com/2007/12/20/drinking-green-tea-daily-lowers-prostate-cancer-risk/ |
|
Back To Top |
|
Mixed Fruit Juice reduces
Prostate Cancer Risk |
Researchers have conducted a study
which has found that drinking a
mixed fruit juice containing fruits
like blueberry, grape and raspberry
on a daily basis can cut the risk of
prostate cancer.
According to lead researcher Dr.Jas
Singh of Sydney University, “We have
undertaken efficacy studies on
individual components of fruit
drinks and found these are effective
in suppressing cell growth in
culture. We reasoned that
synergistic or additive effects are
likely to be achieved when they are
combined.”
The researchers came to this
conclusion after they observed the
effects of the mixed fruit drinks on
both cancer cell cultures in a
laboratory and genetically
engineered mice with human prostate
tumors.
They found that after just two weeks
of consuming the mixed fruit juice
solution which was added to the lab
mice’s drinking water, their tumors
had shrunk by 25%.
Further, the researchers are
planning to see whether a daily
glass or two of this very drink
could treat the disease and even
help to prevent the tumor from
developing. For this, they are
planning a small study of 150 men
with prostate cancer who will be
made to drink three glasses of the
juice everyday.
According to Debbie Clayton of the
Prostate Cancer Charity, “These
studies will need to involve much
larger numbers of men and it may be
several years before we are able to
offer men clear guidance on how the
drink may help them. In the
meantime, we would recommend that
men include a variety of fresh fruit
and vegetables in their diet,
ensuring they get a ‘rainbow’ of
colors.” |
|
Article Source: http://www.healthjockey.com/2007/12/10/mixed-fruit-juice-reduces-prostate-cancer-risk/ |
|
Back To Top |
|
More deaths if no prostate
cancer therapy |
DETROIT, June 2 (UPI) -- Prostate
cancer patients who refuse treatment
don't do as well as those who choose
radiation treatment, U.S.
researchers found.
Researchers at Henry Ford Hospital
in Detroit found the 10-year overall
survival rate for men who chose
"watchful waiting" was 51 percent.
It was 68 percent for those who had
radiation treatment.
"Surgery has been shown to offer a
survival advantage to patients with
prostate cancer when compared with
other treatment options," lead
author Dr. Naveen Pokala of Henry
Ford Hospital said in a statement.
"However, a significant number of
patients refuse surgery and instead
opt for other treatments such as
radiotherapy."
Pokala and colleagues examined
national data of 9,704 male patients
with a mean age of 64.4, and of whom
77 percent were white and 16.4
percent black. Nearly 30 percent
refused any treatment, while 70
percent chose radiation therapy.
The study was presented at the
American Urology Association's
annual meeting in San Francisco. |
|
Article Source: http://www.upi.com/Health_News/2010/06/02/More-deaths-if-no-prostate-cancer-therapy/UPI-71111275526401/ |
|
Back To Top |
|
What Dennis Hopper's Death Can Teach
Us About Prostate Cancer |
Article by Toni Brayer MD
(June 01, 2010) in Health
When Dennis Hopper died of prostate
cancer at age 74, my husband asked
me, "Hey, I thought prostate cancer
didn't kill men and it is slow
growing." Well, he is right about it
usually being slow growing, but
prostate cancer is still the 2nd
leading cause of cancer death in
men. His question made me realize
that there are some facts that
everyone should know about prostate
cancer.
Prostate cancer is very rare in men
under age 40, and the incidence
increases with age. African-American
men are at higher risk, and Asian
and Latin men are less likely than
white guys to get it. We do not know
why these ethnic differences occur.
Family history is important, and men
with an affected brother or father
are twice as likely to get prostate
cancer. Although genes are
undoubtedly responsible, there are
no genetic tests that can predict
it. Some studies show obese men and
men who eat large quantities of red
meat and dairy products are more at
risk. A vasectomy doesn't seem to
matter, nor does exercise or prior
prostatitis.
Prostate cancer grows slowly, and
the PSA (prostate specific antigen)
test or a digital rectal exam can
screen for an enlarged prostate. The
PSA test can be false positive for
many reasons, and the only way to
diagnose suspected prostate cancer
is by a biopsy. The most important
marker for a cancer in the prostate
is the "Gleason" score. This grade
(1-10) tells us how advanced or
aggressive the cancer is. The
pathologist can see if the cells are
suspicious for atypical changes or
are high-grade. The extent of the
tumor determines the stage.
Once a cancer has been diagnosed,
graded and staged, the confusing
choices of treatment come into play.
Because most prostate cancer occurs
in older men and it is slow growing,
many men choose "watchful waiting".
By following PSA tests and
ultrasounds, we can determine if the
cancer is growing. For many men,
nothing more needs to be done,
because the cancer causes them no
problems. For younger men or men
with high Gleason scores, treatment
is usually surgical removal of the
prostate or radiation of the
prostate gland. Radiotherapy can
also occur with seed implantation of
radioactive material. Hormone
therapy or cryoablation is also used
less often.
The Prostate Cancer Foundation and
the Mayo Clinic have more good info
if you wish to delve further.
RIP, Dennis Hopper. I think I'll
take a stroll down memory lane and
rent "Easy Rider" again. I haven't
seen it for 40 years! |
|
Article Source: http://www.opposingviews.com/i/what-dennis-hopper-s-death-can-teach-us-about-prostate-cancer |
|
Back To Top |
|
Prostatic Adenocarcinoma |
Adenocarcinoma of the prostate is
common. It is the most common
non-skin malignancy in elderly men.
It is rare before the age of 50, but
autopsy studies have found prostatic
adenocarcinoma in 80% of men more
than 80 years old. Many of these
carcinomas are small and clinically
insignificant. However, some are
not, and prostatic adenocarcinoma is
second only to lung carcinoma as a
cause for tumor-related deaths among
males. (Bostwick et al, 2004)
Men with a higher likelihood of
developing a prostate cancer (in the
U.S.) include those of older age,
black race, and family history.
Those with an affected first-degree
relative have a much greater risk. (Bostwick
et al, 2004)
Prostate cancers may be detected by
digital examination, by
ultrasonography (transrectal
ultrasound), or by screening with a
blood test for prostate specific
antigen (PSA). None of these methods
can reliably detect all prostate
cancers, particularly the small
cancers. Widespread PSA screening is
not cost-effective. Men whose life
expectancy is less than 10 years not
pursue prostate cancer early
detection because the likelihood of
benefitis outweighed by the risk of
harms from treatment. Men at higher
risk for prostate cancer at earlier
ages, including men of African
American ancestry or a family
history of prostate cancer in
nonelderly relatives, should be
provided the opportunity for
informed decision making at an
earlier age than average-risk men.
(Wolf et al, 2010)
PSA is a glycoprotein produced
almost exclusively in the epithelium
of the prostate gland. In the
circulation PSA may be complexed to
serum proteins (complexed PSA, or
cPSA) or may be free (fPSA). The
cPSA and fPSA together comprise
total PSA (tPSA). The tPSA is
normally less than 4 ng/mL (normal
ranges vary depending upon which
assay is used). A mildly increased
tPSA in a patient with a very large
prostate can be due to nodular
hyperplasia, or to prostatitis,
rather than carcinoma. The fPSA
correlates more closely with benign
prostatic conditions than the tPSA.
The cPSA has a greater sensitivity
for prostatic adenocarcinomas at the
low ranges of elevation. A rising
tPSA is suspicious for prostatic
carcinoma, even if the tPSA is in
the normal range. Transrectal needle
biopsy, often guided by ultrasound,
is useful to confirm the diagnosis,
although incidental carcinomas can
be found in transurethral resections
for nodular hyperplasia. (Jung et
al, 2006)
Men who have findings suspicious for
carcinoma on digital rectal
examination and a tPSA of <4 ng/mL
have a probability of cancer of at
least 10%, while those with tPSA
levels from 4 to 10 ng/mL have a 25%
probability. Men with tPSA's above
10 ng/mL have a >50% likelihood of
having a prostate cancer. (Demura et
al, 1996)
Prostatic adenocarcinomas are
composed of small glands that are
back-to-back, with little or no
intervening stroma. Cytologic
features of adenocarcinoma include
enlarged round, hyperchromatic
nuclei that have a single prominent
nucleolus. Mitotic figures suggest
carcinoma. Less differentiated
carcinomas have fused glands called
cribriform glands, as well as solid
nests or sheets of tumor cells, and
many tumors have two or more of
these patterns. Prostatic
adenocarcinomas almost always arise
in the posterior outer zone of the
prostate and are often multifocal.
(Pearson et al, 1996)
Prostatic adenocarcinomas are
usually graded according to the
Gleason grading system based on the
pattern of growth. There are 5
grades (from 1 to 5) based upon the
architectural patterns.
Adenocarcinomas of the prostate are
given two grade based on the most
common and second most common
architectural patterns. These two
grades are added to get a final
grade of 2 to 10. The stage is
determined by the size and location
of the cancer, whether it has
invaded the prostatic capsule or
seminal vesicle, and whether it has
metastasized.
The grade and the stage correlate
well with each other and with the
prognosis. The prognosis of
prostatic adenocarcinoma varies
widely with tumor stage and grade.
Cancers with a Gleason score of <6
are generally low grade and not
aggressive. Advanced prostatic
adenocarcinomas typically cause
urinary obstruction, metastasize to
regional (pelvic) lymph nodes and to
the bones, causing blastic
metastases in most cases. Metastases
to the lungs and liver are seen in a
minority of cases. (Gleason, 1992) (Bostwick,
1996) (Epstein, 2010)
|
American Urological Society
Clinical Staging
|
|
Stage |
Definition |
10-year Survival
|
|
A1 |
Incidental, <5% of volume
|
93-98% |
|
A2 |
Incidental, >5% of volume,
or high grade |
50% |
|
B1 |
Palpable nodule in one lobe
but <1.5 cm in diameter
|
70-75% |
|
B2 |
Larger palpable nodule
|
62% |
|
C1 |
Invades capsule of prostate
|
40-50% |
|
C2 |
Invades seminal vesicle
|
33-39% |
|
D1 |
Metastases to regional lymph
nodes, or extensive regional
spread |
17-20% |
|
D2 |
Evident distant metastases |
|
|
Article Source: http://library.med.utah.edu/WebPath/TUTORIAL/PROSTATE/PROSTATE.html |
|
Back To Top |
|
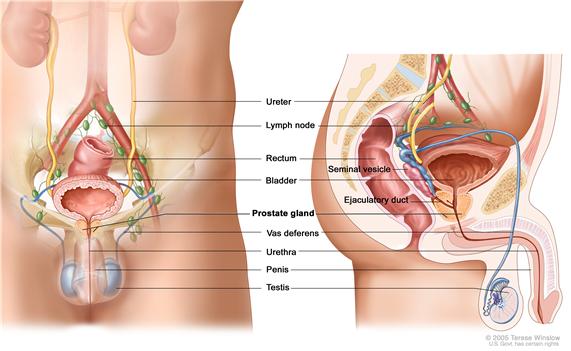
Pathophysiology |
Prostate cancer is classified as an
adenocarcinoma, or glandular cancer,
that begins when normal
semen-secreting prostate gland cells
mutate into cancer cells. The region
of prostate gland where the
adenocarcinoma is most common is the
peripheral zone. Initially, small
clumps of cancer cells remain
confined to otherwise normal
prostate glands, a condition known
as carcinoma in situ or prostatic
intraepithelial neoplasia (PIN).
Although there is no proof that PIN
is a cancer precursor, it is closely
associated with cancer. Over time,
these cancer cells begin to multiply
and spread to the surrounding
prostate tissue (the stroma) forming
a tumor. Eventually, the tumor may
grow large enough to invade nearby
organs such as the seminal vesicles
or the rectum, or the tumor cells
may develop the ability to travel in
the bloodstream and lymphatic
system. Prostate cancer is
considered a malignant tumor because
it is a mass of cells that can
invade other parts of the body. This
invasion of other organs is called
metastasis. Prostate cancer most
commonly metastasizes to the bones,
lymph nodes, rectum, and bladder.
The prostate is a zinc accumulating,
citrate producing organ. The protein
ZIP-1 is responsible for the active
transport of zinc into prostate
cells. One of zinc's important roles
is to change the metabolism of the
cell in order to produce citrate, an
important component of semen. The
process of zinc accumulation,
alteration of metabolism, and
citrate production is energy
inefficient, and prostate cells
sacrifice enormous amounts of energy
(ATP) in order to accomplish this
task. Prostate cancer cells are
generally devoid of zinc. This
allows prostate cancer cells to save
energy not making citrate, and
utilize the new abundance of energy
to grow and spread. The absence of
zinc is thought to occur via a
silencing of the gene that produces
the transporter protein ZIP-1. ZIP-1
is now called a tumor suppressor
gene product for the gene SLC39A1.
The cause of the epigenetic
silencing is unknown. Strategies
which transport zinc into
transformed prostate cells
effectively eliminate these cells in
animals. Zinc inhibits NF-κB
pathways, is anti-proliferative, and
induces apoptosis in abnormal cells.
Unfortunately, oral ingestion of
zinc is ineffective since high
concentrations of zinc into prostate
cells is not possible without the
active transporter, ZIP-
Journal-molecular cancer, review,
2006 5:17,
doi:10.1186/1476-4598-5-17
RUNX2 is a transcription factor that
prevents cancer cells from
undergoing apoptosis thereby
contributing to the development of
prostate cancer.
The PI3k/Akt signaling cascade works
with the transforming growth factor
beta/SMAD signaling cascade to
ensure prostate cancer cell survival
and protection against apoptosis.
X-linked inhibitor of apoptosis (XIAP)
is hypothesized to promote prostate
cancer cell survival and growth and
is a target of research because if
this inhibitor can be shut down then
the apoptosis cascade can carry on
its function in preventing cancer
cell proliferation. Macrophage
inhibitory cytokine-1 (MIC-1)
stimulates the focal adhesion kinase
(FAK) signaling pathway which leads
to prostate cancer cell growth and
survival.
The androgen receptor helps prostate
cancer cells to survive and is a
target for many anti cancer research
studies; so far, inhibiting the
androgen receptor has only proven to
be effective in mouse studies.
Prostate specific membrane antigen (PSMA)
stimulates the development of
prostate cancer by increasing folate
levels for the cancer cells to use
to survive and grow; PSMA increases
available folates for use by
hydrolyzing glutamated folates. |
|
Article Source:http://en.wikipedia.org/wiki/Prostate_cancer |
|
Back To Top |
|
Prostate Cancer Hormone Therapy May
Prove Successful in Treatment of
Surgery-Resistant Cancer |
Recent research into the efficacy of
a new form of hormone therapy for
patients with a certain type of
prostate cancer has yielded
encouraging results, according to a
study published April 15, 2010 in
The Lancet.
The results indicate that the new
hormone treatment, known as MDV3100,
demonstrates "encouraging antitumor
activity in patients with
castration-resistant prostate
cancer," a form of the cancer
resistant to the surgical removal of
the testicles.
The study involved 140 American with
castration-resistant prostate cancer
who were given varying doses of
MDV3100, ranging from 30 to 600
milligrams of the medication daily.
Researchers noted that the primary
objective of the trial was to
"identify the safety and
tolerability profile of MDV3100 and
to establish the maximum tolerated
dose," which was determined to be
240 milligrams of the medication.
Prostate cancer becomes
castration-resistant when cancerous
cells continue to grow, re-grow and
thrive without as much testosterone,
which allows the tumors in the
prostate to mature.
It is not clear whether or not the
treatment will receive federal
approval, as only two of the three
required research phases have been
completed. Completion of the third
phase is underway, with researchers
working to compare the treatment to
a placebo to determine if the
therapy prolongs the life of men
with prostate cancer. |
|
Article Source: http://www.drugwatch.com/news/2010/04/15/prostate-cancer-hormone-therapy-may-prove-successful-treatment-surgery-resistant-can/ |
|
Back To Top |
|
Prostate cancer patients with
low-risk tumors could hold off
treatment |
With the advent of PSA (prostate
antigen) screening nearly 20 years
ago, doctors started to detect
prostate cancers at much earlier
stages. This was explained by
corresponding author Dr. Martin
Sanda, Director of the Prostate
Cancer Center at BIDMC and Associate
Professor of Surgery at Harvard
Medical School.
Dr Martin Sanda commented,
“Consequently, while PSA testing has
enabled us to successfully begin
aggressive treatment of high-risk
cancers at an earlier stage, it has
also resulted in the diagnosis of
cancers that are so small they pose
no near-term danger and possibly no
long-term danger.”
Sanda, jointly with coauthors from
Brigham and Women’s Hospital, the
Harvard School of Public Health and
the University of California, San
Francisco, checked the Health
Professionals Follow-Up Study which
is a big cohort study including
about 51,529 men who have apparently
been followed since 1986. Every two
years, the participants supposedly
replied to questionnaires about
diseases and health-related topics,
as well as whether they have been
diagnosed with prostate cancer.
A sum of about 3,331 men apparently
accounted to receive a diagnosis of
prostate cancer between 1986 and
2007. Additional study discovered
that among this sub-group, about 342
men, just over 10 percent had
apparently chosen to postpone
treatment for one year or longer.
After 10 to 15 years, half of the
men who had primarily delayed
treatment apparently still had not
gone through any treatment for
prostate cancer.
Sanda explained, “We wanted to find
out how this group of men fared in
the long-term. So we looked at the
data they provided us at an average
of eight years after their initial
diagnosis, and compared it with data
provided by prostate-cancer patients
who had opted for aggressive
treatment, such as surgery,
radiotherapy or hormonal therapy. We
found that the deaths attributed to
prostate cancer were very low among
the men with low-risk tumors. Our
analysis showed that only two
percent of the men who deferred
treatment eventually died of the
disease, compared with one percent
of the men who began treatment
immediately following their
diagnosis. This is not a
statistically significant
difference.”
The three types of prostate cancer
were identified as high risk, which
may be big, quicker growing cancers,
intermediate risk and low-risk,
which could be small and slower
growing cancers. There is apparently
plenty of proof that treating
intermediate and high-risk cancers
with surgery, radiation or hormone
therapy may save lives. But how to
take care for low-risk cancer
supposedly is not certain.
Sanda remarked, “These findings
showed that men diagnosed with
low-risk tumors who deferred
treatment were still doing fine an
average of eight years ― and up to
20 years ― following their
diagnosis. In fact, only half of
these men wound up undergoing any
treatment 10 to 15 years
post-diagnosis. This means that they
were able to avoid the disruption in
their quality of life which might
have occurred had they undergone
immediate treatment.”
Sanda adds, “If this approach was
more broadly accepted as a standard
care option for suitable low-risk
prostate cancers, it might help us
avoid throwing the baby out with the
bathwater when it comes to the PSA
test. Instead of just abandoning the
PSA test because it might be leading
to an overdiagnosis of prostate
cancer, we could conduct PSA
screening in a way that allows more
aggressive prostate cancers to be
treated, while less aggressive
tumors could initially be
monitored.”
Sanda believes that this would avoid
problems due to treatment of
‘overdiagnosed’ low-risk cancers,
while preserving the life saving
benefits of treating aggressive
cancers that have been detected
through PSA testing. |
|
Article Source: http://www.healthjockey.com/2009/09/15/prostate-cancer-patients-with-low-risk-tumors-could-hold-off-treatment/ |
|
Back To Top |
|
Ultra-sensitive test to tell
prostate cancer patients if they are
cured after operation |
Scientists are developing an
ultra-sensitive test which will
accurately predict whether men with
prostate cancer are cured after
surgery.
The test should allow doctors to
tell patients that the cancer has
been completely removed, or
recommend further treatment to stop
it coming back.
It is 300 times more reliable than
current commercial tests that
measure levels of protein called PSA
(prostate-specific antigen) in the
blood.
Men who have had their cancerous
prostate gland removed are checked
for PSA, which signals the presence
of cancer cells that may have spread
to the rest of the body.
But existing tests often fail to
detect these cells, resulting in
cancer recurring in 40 per cent of
patients who had been given the
all-clear.
The new VeriSens test uses
nanoparticle-based technology that
appears to more accurately chart the
course of the disease after surgery.
It may pick up cancer recurrence
earlier, when secondary treatment is
more effective for a patient's
survival.
The study results were released
yesterday by scientists at Chicago's
Northwestern University Feinberg
School of Medicine and the
University International Institute
for Nanotechnology.
Co-principal investigator Dr C. Shad
Thaxton said: 'This test may provide
early and more accurate answers.
'It detects PSA at levels in the
blood that cannot be detected by
conventional tests.
'It may allow physicians to act at
the earliest and most sensitive
time, which will provide the patient
with the best chance of long-term
survival.'
Dr Thaxton said the next step for
scientists was a clinical trial to
compare the nano-particle PSA test
to traditional PSA tests and
determine if earlier detection and
treatment can save lives.
Fellow researcher Dr William
Catalona added: 'It should be
especially useful in the early
identification of men who would
benefit from postoperative radiation
therapy and those who need
postoperative salvage radiation
therapy for recurrence.'
John Neate, chief executive of the
Prostate Cancer Charity, said: 'This
new study describes a new diagnostic
tool, a nanoparticle-based PSA test,
which appears to give very accurate
PSA readings at much lower levels
than the standard follow-up tests
currently used.
'It is too soon to know whether the
test will have a place in clinical
practice.
'Only through further studies would
the researchers be able to identify
whether being able to detect the
return of prostate cancer at an
earlier stage would have the desired
effect of improving long-term
survival.' |
|
Article Source: http://www.dailymail.co.uk/health/article-1283472/Prostate-cancer-test-let-patients-know-cured-operation.html?ITO=1490 |
|
Back To Top |
|
Sound waves prostate cancer
treatment may have lesser side
effects on the patient |
Prostate cancer may now be
effectively treated in a
non-invasive manner, which may even
result in lesser side effects. Such
a treatment is believed to be
possible through an experimental
cancer therapy, called the
High-Intensity-Focused Ultrasound (HIFU).
This therapy, which uses sound waves
to destroy the tumor cells, is
believed to have been tested in a
trial conducted in London at the
University College Hospital and the
Princess Grace Hospital.
The study experts have explained
that HIFU is a therapy which uses
high frequency sound waves to heat a
specific area to the temperature of
about 80-90◦C. This therapy may
possibly be used to treat either the
entire prostate or merely a specific
targeted cancer region.
Men suffering from prostate cancer
may usually be treated with either
radiotherapy or surgery. Often
surgery may require the patient to
stay in the hospital for a period of
2-3 days; while radiotherapy may
notably require daily treatment as
an outpatient for atleast 1 month.
Thereby, in order to better
understand the effect of the HIFU
therapy on patients with prostate
cancer, the study investigators
notably tested this therapy on more
than 150 such patients. It was
further also stated that these
patients were treated with this
particular therapy under general
anesthesia. The experts have stated
that five hours after receiving the
HIFU therapy, the patients were
evidently discharged from the
hospitals.
More so, out of some of the patients
which were followed for a year,
around 92% of them didn’t seem to
re-experience prostate cancer. Even
though it was noted that this study
may not be a comparative study, it
is presumed that the presently used
treatments may reveal similar
statistics of men showing no
recurrence of the disease after one
year.
Lead study expert, Dr. Hashim Ahmed,
UCL’s division of surgical and
interventional science, says that,
“This study suggests it’s possible
that HIFU may one day play a role in
treating men with early prostate
cancer with fewer side effects. But
we don’t yet know for sure if HIFU
is more effective than traditional
treatments so it will be important
to carry out further studies
involving a larger number of
patients followed over a longer
period of time to truly compare the
long term effectiveness of this
treatment.”
Apart from this, Professor Peter
Johnson, chief clinician at the
Cancer Research UK, says that, “This
technique needs careful evaluation
to make sure that it can produce the
same results as the proven
treatments for early prostate
cancer. If the treatment can be
shown to have less side effects then
that will be excellent news, but
more research is needed to show
this. Cancer Research UK is funding
a trial to look at this question and
we hope that further studies can be
carried out to compare HIFU to
standard treatments.”
Out of the patients followed for one
year after their HIFU therapy, it
was observed that 1 man had
incontinence, while around 30-40% of
them had impotence. On the other
hand, neither of the patients was
noted to experience any
bowel-related issues. In contrast to
this, a different ratio was presumed
to take place for the patients who
may either undergo surgery or
radiotherapy. It was presumed that
around 5-20% of these patients may
experience incontinence, while
almost 50% may have impotence. Apart
from this, around 5-20% of the
patients may even experience various
other ill-effects of radiotherapy
like pain, bleeding and diarrhea. |
|
Article Source: http://www.healthjockey.com/2009/07/02/sound-waves-prostate-cancer-treatment-may-have-lesser-side-effects-on-the-patient/ |
|
Back To Top |
|
Why you should consider a
prostate cancer PSA test today |
Prostate cancer kills if allowed to
grow. If ever there was a good
reason to have a simple blood test,
this is it. The prostate cancer PSA
(prostate specific antigen) test is
one of the tests given to determine
if cancer cells are present in an
otherwise healthy prostate. It is a
simple blood test to help doctors
diagnose and identify the existence
of prostate cancer.
The PSA test, although considered a
prostate-specific test, is not
really an absolute definitive test
for the cancer. Depending on the
research conducted, the PSA test is
known to be somewhere between 85 and
95 percent accurate in identifying
prostate cancer.
While an elevated PSA test may
suggest the presence of prostate
cancer, it’s not an absolute.
However, if you have an elevated
result, your doctor will probably
want to do additional testing for a
more complete and accurate
assessment of the potential cancer.
The last thing you want to do is to
allow prostate cancer to grow beyond
the prostate gland.
The good news is that benign
prostatic hyperplasia (BPH), better
known as an enlarged prostate, can
also elevate the PSA test results.
Even prostatitis and lower urinary
tract symptoms can show elevated
levels of PSA, so if you have an
elevated test result, don’t panic. A
normal result from a PSA test
doesn’t guarantee that you’re free
from cancer, nor does a
higher-than-normal result mean you
do have cancer.
It’s critical that you follow your
doctor’s lead in regard to dealing
with the PSA test results. The
results are an indication, and
should be used as a tool to develop
a complete diagnosis. To complicate
matters more, PSA levels can also
increase with age. The relative size
of your prostate also plays a factor
in interpreting the results.
As many as two out of three people
with elevated PSA readings do not
have a malignancy.
TEST BENEFITS
Here’s a quick list of the benefits
and reasons why you should consider
getting a PSA test:
1. It’s possible to detect a
cancerous condition before any
symptoms are known.
2. Early detection catches prostate
cancer before it has spread,
increasing the chances of a complete
cure.
3. The PSA blood test has been
recognized as a contributing factor
that has significantly reduced the
number of prostate cancer deaths.
While the PSA test can also deliver
a false positive about 20 percent of
the time, it is recognized as a good
indicator of potential cancerous
conditions and should be taken
seriously.
A 2005 Harvard study indicated that
men having an annual PSA test were
almost three times less likely to
die of prostate cancer than men who
didn’t bother with the test. So, the
best reason to have the test is that
without it, you greatly increase the
chances of dying from prostate
cancer. |
|
Article Source: http://www.silive.com/healthfit/index.ssf/2010/05/why_you_should_consider_a_prostate_cancer_psa_test_today.html |
|
Back To Top |
| |
|
|
|
|

